
Diabetic retinopathy (DR) is a significant health concern and a common microvascular complication of diabetes mellitus (DM). It specifically affects the eyes, damaging the retina, and stands as a leading cause of vision loss and irreversible blindness, particularly among working-age adults and individuals over 50 yrs. This condition is characterized by progressive damage to the retinal microvasculature.
Causes of diabetic retinopathy:
- Chronic hyperglycemia, a hallmark of diabetes, triggers a cascade of biochemical and physiological alterations that culminate in retinal microvascular damage.
- The polyol pathway plays a key role in DR development. In hyperglycemia, excess glucose is converted to sorbitol by aldose reductase, and then to fructose by sorbitol dehydrogenase (SDH).The accumulation of sorbitol and fructose causes osmotic stress, oxidative stress, and the production of advanced glycation end products (AGEs). The accumulation of AGEs further amplifies the inflammatory response and promotes microvascular dysfunction.
- Inflammation is a critical factor in DR pathogenesis, contributing to endothelial dysfunction, microvascular damage, and increased vascular permeability. Hyperglycemia-induced oxidative stress and endothelial dysfunction may underlie observed inflammatory markers.
- Metabolic dysregulation, including dyslipidemia (abnormal blood lipid levels), is an important risk factor for DR development and progression. Elevated triglyceride levels are associated with an increased risk of DR, while higher HDL cholesterol levels are linked to a reduced risk.
- Insulin resistance (IR) is fundamental to Type 2 DM and leads to blood sugar and lipid metabolism disturbances, damaging tissues and organs.
- Extraocular factors contributing to DR risk and progression include inadequate glycemic control, hypertension, dyslipidemia, the duration of diabetes, pregnancy, and genetic predispositions.
- Obstructive sleep apnea syndrome (OSAS), characterized by repeated episodes of partial or complete upper airway blockage during sleep, is linked to the severity of macular edema in DR patients. OSAS causes intermittent hypoxia, leading to sympathetic activation, elevated inflammatory markers, endothelial damage, oxidative stress, and VEGF release, accelerating retinal vascular damage.
- Higher urinary levels of certain caffeine metabolites have been associated with an increased risk of DR in US males with diabetes.
- Osteoarthritis (OA) is linked to metabolic disorders and inflammation. Joint replacement surgery in OA patients is associated with a reduced risk of developing DR, which researchers hypothesize may be due to reduced systemic inflammation.
- The loss of pericytes, supporting capillary integrity, is a hallmark of early DR, potentially mediated by the polyol pathway, leading to capillary instability, microaneurysm formation, and blood-retinal barrier breakdown.
Signs and Symptoms of diabetic retinopathy:
- DR often presents insidiously in its early stages, with no obvious symptoms of vision impairment.
- Visual impairment typically indicates disease progression to advanced stages3.
- Macular edema (ME), the accumulation of fluid in the macula, is one of the leading causes of visual loss in DR.

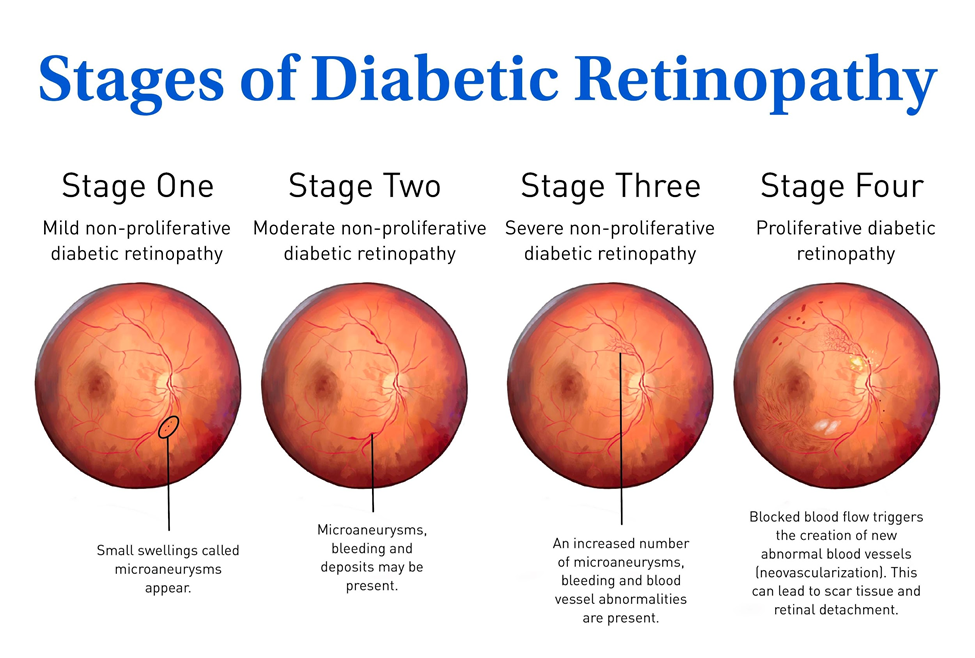
- Proliferative diabetic retinopathy (PDR), a severe stage, is characterized by neovascularization (growth of new blood vessels). These new vessels are often fragile and leaky, leading to hemorrhage and vision loss. PDR can result in severe complications like vitreous hemorrhage (VH), fibroproliferative membranes, and tractional retinal detachment.VH is common in PDR and can cause severe vision loss.
- Patients with DR and cataracts may experience difficulties with pupil dilation and postoperative pupil abnormalities, which can limit fundus visibility and complicate postoperative monitoring and diagnosis.
Diagnosis of diabetic retinopathy:
- DR detection involves clinical examinations and advanced imaging technologies.
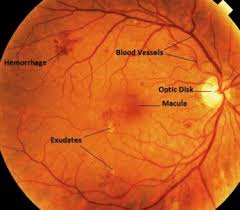
- Ophthalmologists use fundus images and fluorescein angiography (FFA) to identify signs like hemorrhages, microaneurysms, and exudates. FFA provides visualization of retinal vascular morphology, leakage, and hemodynamic changes, aiding in disease staging, macular edema assessment, and treatment monitoring.
- Optical coherence tomography (OCT) is an essential tool for diagnosing and treating macular edema, providing a cross-sectional view of the retina to identify structural changes and fluid accumulation. OCT angiography (OCTA) can quantify vascular parameters in the retina and choroid.
- An accurate diagnosis relies on a thorough clinical evaluation, including visual acuity testing, fundus examination, and OCT imaging. Medical history is also collected.
- Early detection is crucial for preventing complications. Routine fundus screening is indispensable for individuals with diabetes.
- Automated diagnostic systems using deep learning (AI) are being developed to analyze FFA images for rapid and accurate diagnosis and grading of DR and detection of complications like DM.
- Routine blood parameters, specifically leukocyte differential count ratios like Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Systemic Immune-Inflammation Index (SII), are being explored as potential, cost-effective inflammatory biomarkers to facilitate early DR identification and risk stratification, particularly in settings with limited access to ophthalmologists.
- The triglyceride glucose (TyG) index, a simple measure of insulin resistance, and the Systemic Immune-inflammation Index (SII) may predict the occurrence of DR in patients with Type 2 diabetes, serving as useful adjunct tools for risk stratification and early identification of patients needing more frequent ophthalmologic evaluations. These biomarkers are not substitutes for gold standard diagnostic methods like ophthalmoscopy and retinal imaging.
- Obstructive sleep apnea syndrome (OSAS) is typically diagnosed through overnight polysomnography (PSG).
Treatment of diabetic retinopathy:
Treatment strategies are guided by the stage of the disease.
- For non-proliferative stages (NPDR), treatment options include pharmacologic intervention and laser therapy.
- Main treatment options for DR include retinal laser photocoagulation (such as panretinal photocoagulation for PDR or focal/grid macular laser treatment for macular edema).
- Intravitreal injections of anti-vascular endothelial growth factor (anti-VEGF) drugs (such as ranibizumab, bevacizumab, or aflibercept) are widely utilized therapeutic interventions. Anti-VEGF drugs inhibit proangiogenic factors like VEGF-A, VEGF-B, and placental growth factor, counteracting pathological neovascularization and disease progression. Adherence to the scheduled injection regimen is crucial for successful outcomes.
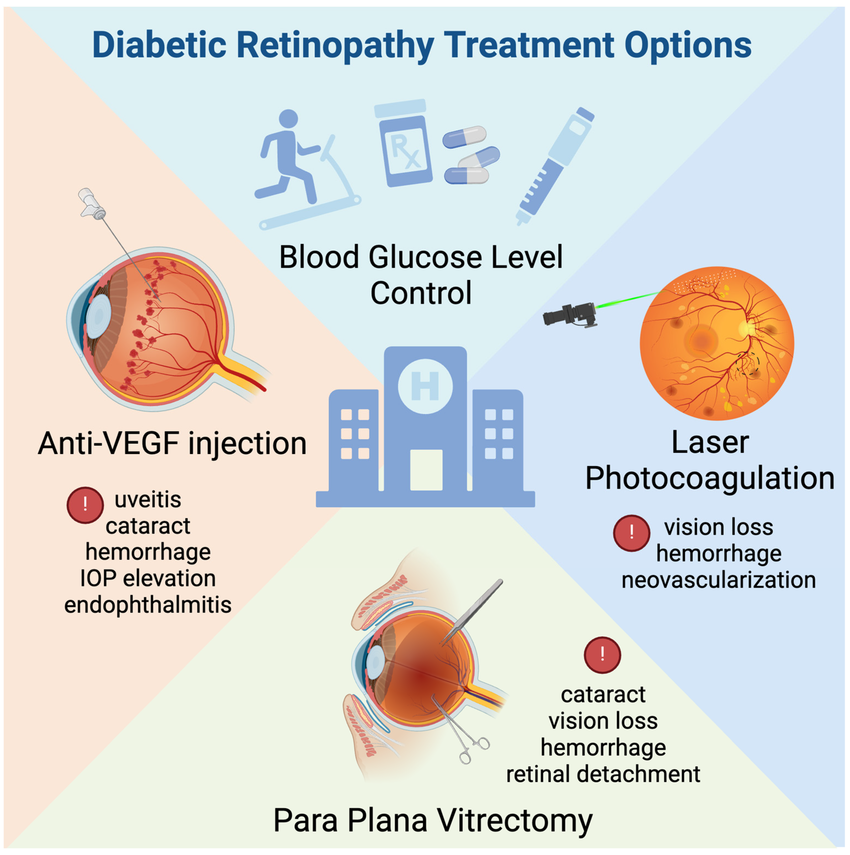
- Vitrectomy surgery is considered the first-line treatment for vision loss caused by vitreous hemorrhage or tractional retinal detachment in advanced stages of DR. Intravitreal anti-VEGF drugs may be injected one week before vitrectomy.
- Strict control of underlying systemic conditions, particularly glycemic control (monitored by HbA1c), hypertension, and dyslipidemia, is paramount in managing DR.
- Emerging therapeutic approaches include epigenetic modification agents, such as DNMT inhibitors, which have been used in DR treatment.
- For patients with both DR and cataracts, phacoemulsification with intraocular lens implantation (PHACO + IOL) is the standard approach for cataract treatment, which can improve vision and allow for better visualization for subsequent retinal treatment.
- Managing concurrent conditions like OSAS may potentially improve treatment outcomes for macular edema.
Prognosis:
- The clinical presentation of visual impairment often indicates that the disease has progressed to advanced stages.
- If proliferative DR is not treated in a timely manner, it may lead to irreversible vision loss. Diabetic macular edema can also significantly impair central vision.
- Postoperative complications can affect the prognosis. Vitreous hemorrhage is common after vitrectomy and can impact vision recovery.
- Patients with OSAS may exhibit a poorer response to anti-VEGF therapy, and the severity of OSAS may have a bearing on the therapeutic response in macular edema.
- Pupillary changes observed after cataract surgery in patients with DR and cataracts can lead to less than ideal vision recovery. Risk factors for these changes include longer diabetes duration, higher lens nucleus grade (hardness), greater DR severity, and intraoperative posterior lens capsule rupture.
- Early detection and effective management of DR are crucial for protecting vision and improving long-term outcomes.
- Biomarkers can help predict prognosis. Quantifying choroidal vascular density (VD) using Widefield Swept-Source OCT Angiography (WSS-OCTA) may help predict DR progression. A decrease in the VD of the superior region in the choriocapillaris layer indicates the onset of PDR and necessitates expeditious treatment to prevent vision-threatening complications. Peripapillary Bruch’s membrane Opening-Minimum Rim Width (BMO-MRW) is reduced in early DR and correlates with microvascular changes, suggesting its potential as a biomarker for monitoring disease progression.
- Despite the availability of treatments, some limitations persist, such as the high cost and invasive nature of certain therapies like anti-VEGF injections.
References:
- Abualhasan H, Beshtawi IM, Hantoli S, Noor M, Mustafa O. Predictive factors for adherence to intravitreal anti-vascular endothelial growth factor therapy in Palestinian patients with diabetic retinopathy, retinal vein occlusion, and age-related macular degeneration: A Retrospective Cohort Study. BMC Ophthalmol. 2025;25:268. doi:10.1186/s12886-025-04113-9.
- Amin R, Ansyori AK, Erna R, Fauzi L. Epigenetic Regulation of Sorbitol Dehydrogenase in Diabetic Retinopathy: A Case Control Study. Biologics: Targets and Therapy. 2025.
- Banerjee L, Karkhur S, Singh P, Verma V, Gupta S, Goyal A. Effect of Obstructive Sleep Apnea Syndrome on Macular Edema Severity and Response to Intravitreal Ranibizumab in Diabetic Retinopathy and Retinal Vein Occlusion. Cureus. 2025;17(3):e81385. doi:10.7759/cureus.81385.
- Chen X, Li J, Guo Q, Xu N, Huang L, Miao H. The association between urinary caffeine and caffeine metabolites and diabetic retinopathy. Sci Rep. 2025.
- Harley O, Amelia YS, Gustianty E, Soetedjo NNM, Kartasasmita AS. Exploring leukocyte differential count ratio profiles as inflammatory biomarkers in diabetic retinopathy: a systematic review and meta-analysis. BMC Ophthalmol. 2025;25:265.
- Huang CT, Law YY, Wang K, Lee CY, Huang JY, Yang SF, et al. Reduced risk of diabetic retinopathy in osteoarthritis patients undergoing joint replacement surgery.
- Long X, Gan F, Fan H, Qin WG, Li X, Ma R, Wang L, et al. EfficientNetB0-Based End-to-End Diagnostic System for Diabetic Retinopathy Grading and Macular Edema Detection. Diabetes, Metabolic Syndrome and Obesity. 2025.
- Raimondi R, Sow K, Peto T, Wride N, Habib MS, Sproule A, et al. The effect of intraocular pressure during phacoemulsification in patients with either diabetic retinopathy or glaucoma; a randomized controlled feasibility trial. Graefes Arch Clin Exp Ophthalmol. 2025.
- Sushith M, Srinivasan A, Ramesh R, Ramkumar P. A hybrid deep learning framework for effective detection and classification of diabetic retinopathy. Sci Rep. 2025.
- Wang J, Su J, Ma J, Liu D. Causal roles of lipids and mediating plasma proteins in diabetic retinopathy: a Mendelian randomization study. Diabetol Metab Syndr. 2025;17:139.
- Zhou J, Wang X, Lou W, Li T, Zhang Y, Hu Y, Long D, et al. Peripapillary Bruch’s membrane Opening-Minimum Rim Width (BMO-MRW) and microvascular changes in early diabetic retinopathy. BMC Ophthalmology. 2025;25:257.
