

Dry eye syndrome (DES), also known as dry eye disease (DED), keratoconjunctivitis sicca (KCS), sicca syndrome, keratitis sicca, xerophthalmia, dysfunctional tear syndrome, or ocular surface disease, is a condition affecting the preocular tear film. It results from damage to the ocular surface and is characterized by symptoms of ocular discomfort.

DED is a multifactorial disorder characterized by a loss of homeostasis in the tear film, accompanied by ocular symptoms. This condition is associated with inflammation of the ocular surface, hyperosmolarity of the tear film, and neurosensory abnormalities.
Diagnostic Tests for Dry Eye Syndrome:
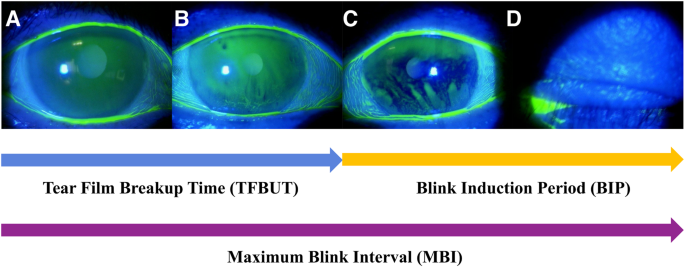
- Tear film break-up time (TBUT or BUT): Measures how long the tear film remains stable before breaking up. A BUT ≤ 5 seconds is included in some diagnostic criteria. A BUT < 10 seconds has been used as an inclusion criterion for studies on persistent dry eye after refractive surgery.
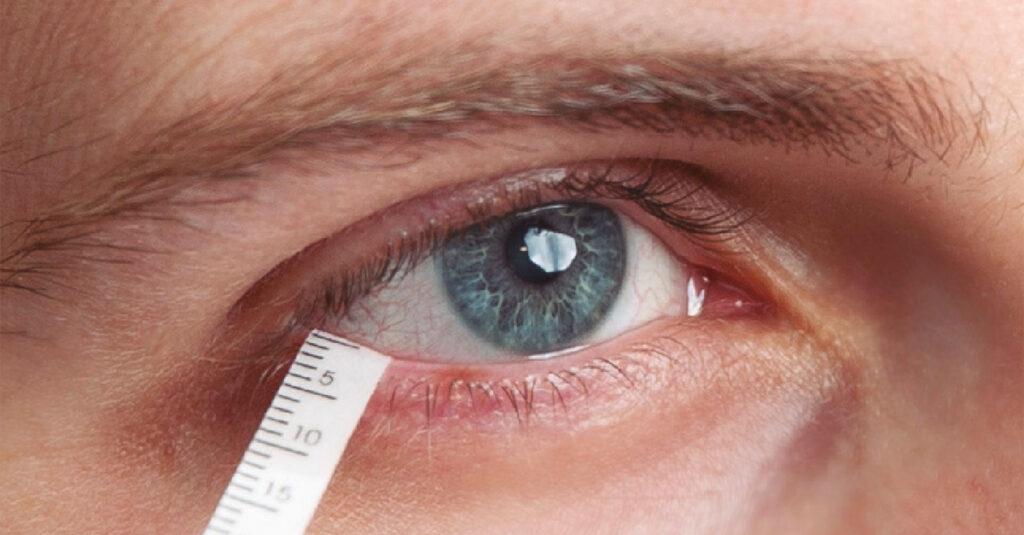
- Schirmer I test (SIT): Measures tear production. A result ≤ 5 mm/5 minutes is part of some diagnostic criteria. A result < 5 mm after 15 minutes is also used. However, the Schirmer test’s reliability in anophthalmic sockets is questionable due to potential tear pooling behind a prosthesis.
- Corneal and conjunctival fluorescein staining score (FS score): Assesses damage to the ocular surface. A score ≥ 5 points is included in some diagnostic criteria.
- Meibomian Gland Evaluation:
- Meibography: Uses infrared photographs of everted eyelids to evaluate the area occupied by meibomian glands. Meibomian gland abnormalities are part of DASS diagnostic criteria.
- Meibomian gland yielding liquid secretion (MGYLS) score: Measures the secretion function of the glands.
- Meibomian secretory function scores (MGS) and number of glands secreting any liquid (MGL).
- Tear Meniscus: A reduced tear meniscus is a contributing factor and diagnostic criterion for DASS. Tear meniscus height (TMH) can be measured, with < 150ɥm being a diagnostic criterion in some cases.
- Ocular Surface Inflammation:
- Clinical conjunctival socket inflammation.
- Increased levels of matrix metalloproteinase-9 (MMP-9). A point-of-care immunoassay for MMP-9 is commercially available.
- Conjunctival hyperemia (redness) can indicate inflammation.
- Tear Film Hyperosmolarity: Included in DASS diagnostic criteria.
- Corneal Nerve Assessment:
- In vivo confocal microscopy (IVCM) can be used to examine corneal nerve morphology, such as nerve fiber length (NFL), nerve fiber density (NFD), and nerve branch density (NBD). Reduced NFL has been observed in patients with dry eyes or diabetes.
- Blink reflex (BR) can assess the function of the corneal nerve closed-loop. An increased R1 Latency of blink reflexes has been found specifically in patients with both dry eyes and diabetes.
- Other Measures:
- Direct assessment of tear secretion (DATS): An objective imaging technology used to measure tear secretion in anophthalmic sockets.
- Measurement of tear film lipid layer thickness (TFLLT) or lipid layer thickness (LLT).
- Tear protein analysis, such as measuring tear lactoferrin levels, can be used for diagnosis. Abnormal protein profiles have been found in the tears of patients with dry eye syndrome.
Management Strategies for Dry Eye Syndrome:
Management strategies for dry eye aim to treat the signs and symptoms and address underlying causes.
General and First-Line Treatments:
- Artificial tears (ocular lubricants): Commonly used to supplement natural tears and provide surface lubrication. Sodium hyaluronate (HA) is a widely used type of artificial tear that helps thicken and stabilize the tear film, reduce mechanical trauma, aid corneal epithelial healing, and prevent hyperosmolality. However, artificial tears may not address the root cause, and prolonged use can potentially lead to corneal epithelial defects.
- Warm compresses: Can enhance meibomian gland function and improve tear quality. Effective for MGD and dry eye, leading to increased tear film lipid layer thickness, TBUT, meibomian gland scores, and complete blink rate. Achieving an optimal temperature is important.
- Eyelid hygiene: Maintaining clean eyelids, often with warm water and shampoo, is essential for ocular surface health and helps reduce meibomian gland obstruction.
- Lifestyle modifications: Reducing computer use can decrease tear film evaporation. Increasing blink repetition is also mentioned.
Medications:
- Topical anti-inflammatory drugs: May be used for patients with severe symptoms.
- Topical Cyclosporine A (CsA): A potent treatment targeting anti-inflammatory effects, approved by the FDA for dry eye disease. While effective, it can be expensive and requires frequent application (e.g., four times daily). Research is exploring sustained-release options.
- Topical Lifitegrast: Also approved by the FDA for dry eye, used for refractory cases. It is expensive and requires twice-daily application. Sustained-release options are being investigated.
- Mucin secretagogues: Such as diquafosol and rebamipide, are used to stabilize the tear film. They stimulate mucin secretion, increase goblet cell numbers, and improve mucosal epithelium. Diquafosol sodium (DQS) promotes hydration and tear film stabilization and can alleviate corneal irregularity and improve optical quality.
Procedures and Therapies:
- Thermal pulsation therapy (TPT): A non-invasive treatment combining heat and massage to alleviate meibomian gland dysfunction (MGD) symptoms. It provides moderate, clinically meaningful improvements in MGYLS scores and TBUT. TPT can be used before, after, or for pre-existing dry eye following cataract surgery to improve tear film stability and gland function. Lipiflow® is an example of TPT.
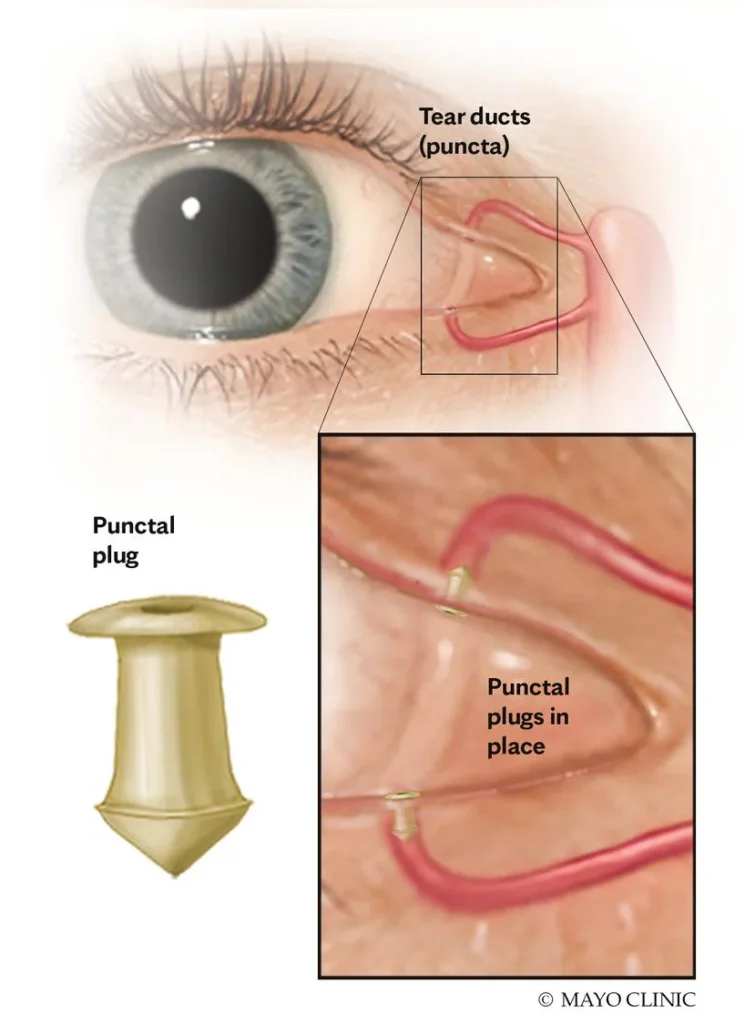
- Punctal plugs: Can be used to relieve symptoms.
- Surgical procedures: For severe symptoms, surgical options like intraductal probing may be considered.
- Electroacupuncture: Explored as a treatment strategy for dry eye in patients with type 2 diabetes mellitus (T2DM).
Addressing Underlying Causes and Risk Factors:
- Diabetes Management: Patients with diabetes should receive appropriate therapy to maintain normal blood sugar levels, which helps minimize the risk of dry eye. High blood sugar negatively impacts tear film function, reduces tear secretion, and activates inflammation.
- Inflammation Management: Addressing elevated inflammation is important. Consuming fiber-rich foods like vegetables, beans, and fruits, which contain vitamins and trace elements, can enhance anti-inflammatory properties.
- Psychological Counseling: Can help manage anxiety and depression, which are associated with dry eye and its risk.
- Smoking Cessation: Smoking increases the risk of postoperative dry eyes; quitting can effectively reduce this risk.
- Surgical Technique: Utilizing smaller surgical incisions may help minimize the risk of dry eye after cataract surgery.
References
- Adrian T, Lubis RR, Zubaidah TSH. Association between Frequency of Prosthesis Cleaning and the Discharge Characteristics and the Tear Film in Subjects with Anophthalmic Socket after Eviceration with Dermis Fat Graft. Open Access Maced J Med Sci. 2018;6:2012–6.
- Albietz JM, Lenton LM, McLennan SG. Chronic dry eye and regression after laser in situ keratomileusis for myopia. J Cataract Refract Surg. 2004;30:675– 84.
- Alves M, Reinach PS, Paula JS, Vellasco e Cruz AA, Bachette L, Faustino J, et al. Comparison of diagnostic tests in distinct well-defined conditions related to dry eye disease. PLOS ONE. 2014;9(5):e97921.
- Amparo F, Schaumberg DA, Dana R. Comparison of two questionnaires for Dry Eye Symptom Assessment: the ocular surface Disease Index and the Symptom Assessment in Dry Eye. Ophthalmology. 2015;122(7):1498–503.
- An J, Wang L, Song S, Tian L, Liu Q, Mei M, Li W, Liu S. Electroacupuncture reduces blood glucose by regulating intestinal flora in type 2 diabetic mice. J Diabetes. 2022;14(10):695–710. doi: 10.1111/1753-0407.13323.
- Ayaki M, et al. Sleep disorders are a prevalent and serious comorbidity in dry eye. Investig Ophthalmol Vis Sci. 2018;59:DES143–DES150. https://doi.org/10.1167/iovs.17-23467.
- Ayaki M, Kawashima M, Negishi K, Tsubota K. High prevalence of sleep and mood disorders in dry eye patients: survey of 1,000 eye clinic visitors. Neuropsychiatr Dis Treat. 2015;11:889–894. https://doi.org/10.2147/ndt.S81515.
- Best N, Drury L, Wolffsohn JS. Predicting success with silicone-hydrogel contact lenses in new wearers. Cont Lens Anterior Eye. 2013;36(5):232-7.
- Blalock TD, Spurr-Michaud SJ, Tisdale AS, Heimer SR, Gilmore MS, Ramesh V, et al. Functions of MUC16 in corneal epithelial cells. Invest Ophthalmol Vis Sci. 2007;48(10):4509–4518. https://doi.org/10.1167/iovs.07-0430 PMID: 17898272.
- Caffery B, Heynen ML, Joyce E, Jones L, Ritter R 3rd, Senchyna M. MUC1 expression in Sjögren’s syn-drome, KCS, and control subjects. Mol Vis. 2010;16:1720–1727. PMID: 20806091.
- Castro JS, Selegatto IB, Castro RS, Vasconcelos JP, Arieta CE, Alves M. Translation and validation of the Portuguese version of a dry eye disease symptom questionnaire. Arq Bras Oftalmol. 2017;80(1):14-6.
- Chalmers RL, Begley CG. Dryness symptoms among an unselected clinical population with and without contact lens wear. Cont Lens Anterior Eye. 2006;29(1):25-30.
- Chen L, Vasudev G, Szeto A, Cheung WY. Trust in doctors and non-doctor sources for health and medical information. J Clin Oncol. 2018;36:10086. 10.1200/JCO.2018.36.15_SUPPL.10086.
- Chen Z, Lin X, Qu B, et al. Preoperative expectations and postoperative outcomes of visual functioning among cataract patients in Urban Southern China. PLoS ONE. 2017;12:e0169844. https://doi.org/10.1371/journal.pone.0169844.
- Chylack LT Jr, Wolfe JK, Singer DM, Leske MC, Bullimore MA, Bailey IL, et al. The Lens Opacities Classification System III. The Longitudinal Study of Cataract Study Group. Arch Ophthalmol. 1993;111(6):831-6
